



 09 Sep 2024
09 Sep 2024 Myopia:
Myopia, or short-sightedness, is a refractive error of the eye where light rays focus in front of the retina rather than directly on it, causing distant objects to appear blurry. This condition can occur due to excessive refractive power of the cornea or lens, or from an elongated eyeball. Myopia brought about by an excessively elongated eyeball is known as axial myopia, and is the most common underlying cause of myopia today.
While the refractive error caused by myopia can be easily corrected with glasses or contact lenses, individuals with high axial myopia face an increased risk of various ocular conditions due to the elongation or “stretching” of the eyeball. These risks include retinal detachment, myopic degeneration, glaucoma, earlier onset of cataracts, and other retinal diseases which are sight-threatening and can lead to blindness. Thus, the eyes of people with myopia are structurally different from those without. Myopia is known to progress rapidly between the ages of 8-15. This highlights the importance of controlling axial length elongation in children and pre-teens.
There has been an increasing prevalence of myopia around the world during the last few decades. The myopia rate of school children in China has increased by 10% from 2006 to 2015. The global rate of myopia is predicted to be 50% in 2050 [1]. Genetic factors are unlikely to affect myopia prevalence so steeply; after all, never before in human history has myopia been so common.
Indeed, there is an unknown fundamental factor in our modern-day environment pushing myopia development.
Causes:
In research for the cause of myopia, it is not surprising that the increase in consumption of near-related activities in our daily lifestyle takes center stage. One can deduce that the increase of near-work activities is one of the leading causes of myopia. The leading theory which supports this is called “hyperopic defocus theory”.
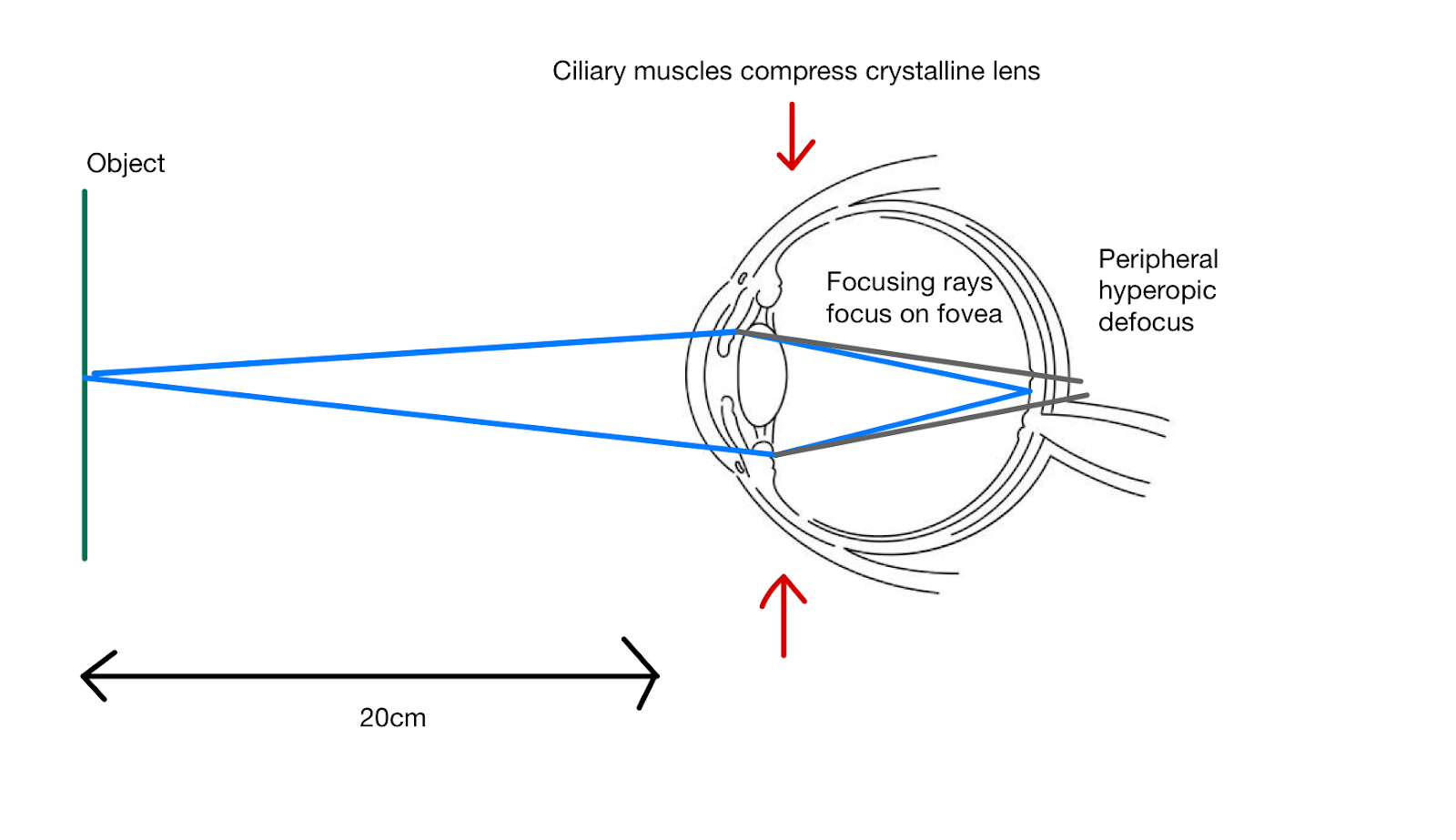
Our eyes can only shift their focus from distance to near. They do this by contracting our ciliary muscles to squeeze the crystalline lens in order to increase its dioptric power. By this mechanism, light is brought into focus onto the foveal region- the focusing point of the eye. However, the peripheral images still lie behind the retina. This is known as hyperopic defocus. It is theorized that hyperopic defocus stimulates the axial growth of the eyeball, leading to myopia [2].
History of Orthokeratology:
In the early days of contact lens technology, large diameter corneal rigid lenses were used. It was found that if the lenses were fitted too flat, the cornea was flattened and reshaped. This led to some patients seeing better than before. It was from these observations that the inventor of Orthokeratology lenses (Ortho-K), George Jensen, came up with the idea to temporarily re-shape the corneas of his patients in order to grant them clear vision. It was Dr Stuart Grant who suggested Ortho-K to be worn overnight so as to provide the user with clear vision during the day.
Mechanism Of Orthokeratology:
Originally, Ortho-K was- and still is- touted as a non-surgical and reversible alternative to refractive surgery. Hence, its main users were adults. As the mechanism of Ortho-K was being studied, it was discovered that the compression effect of the lenses shifted corneal cells from the center to the periphery.
For illustration, Figure A and B below compares the corneal topography scans of a cornea before and during ortho-k treatment.
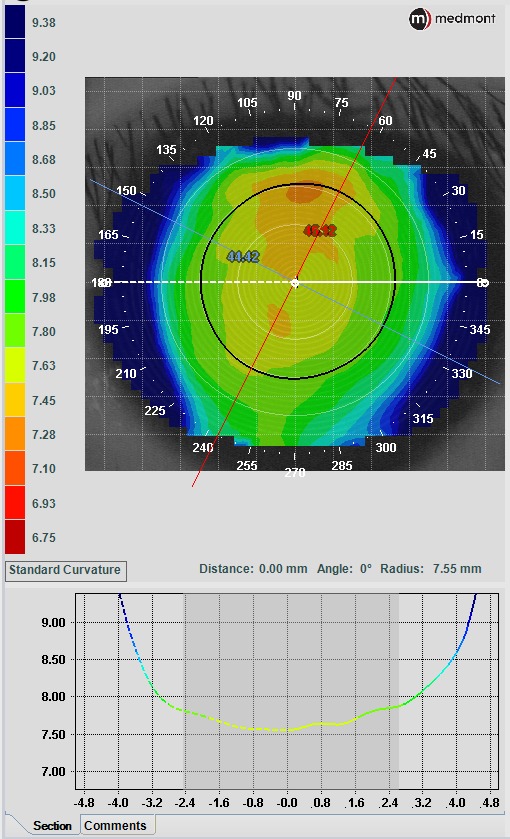
Figure A (Above): Baseline Cornea
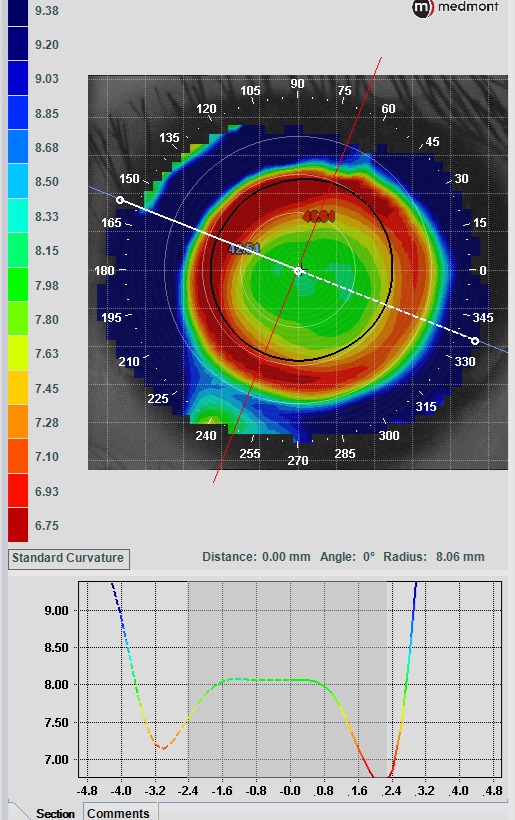
Figure B (Above): Cornea topography during ortho-k treatment
As seen in figures A and B above, during ortho-k treatment, corneal cells move to the periphery, and form a ring around the focal point of the cornea. Incidentally, this creates a peripheral blur. This eliminates the peripheral hyperopic defocus that is theorized to stimulate axial length growth.
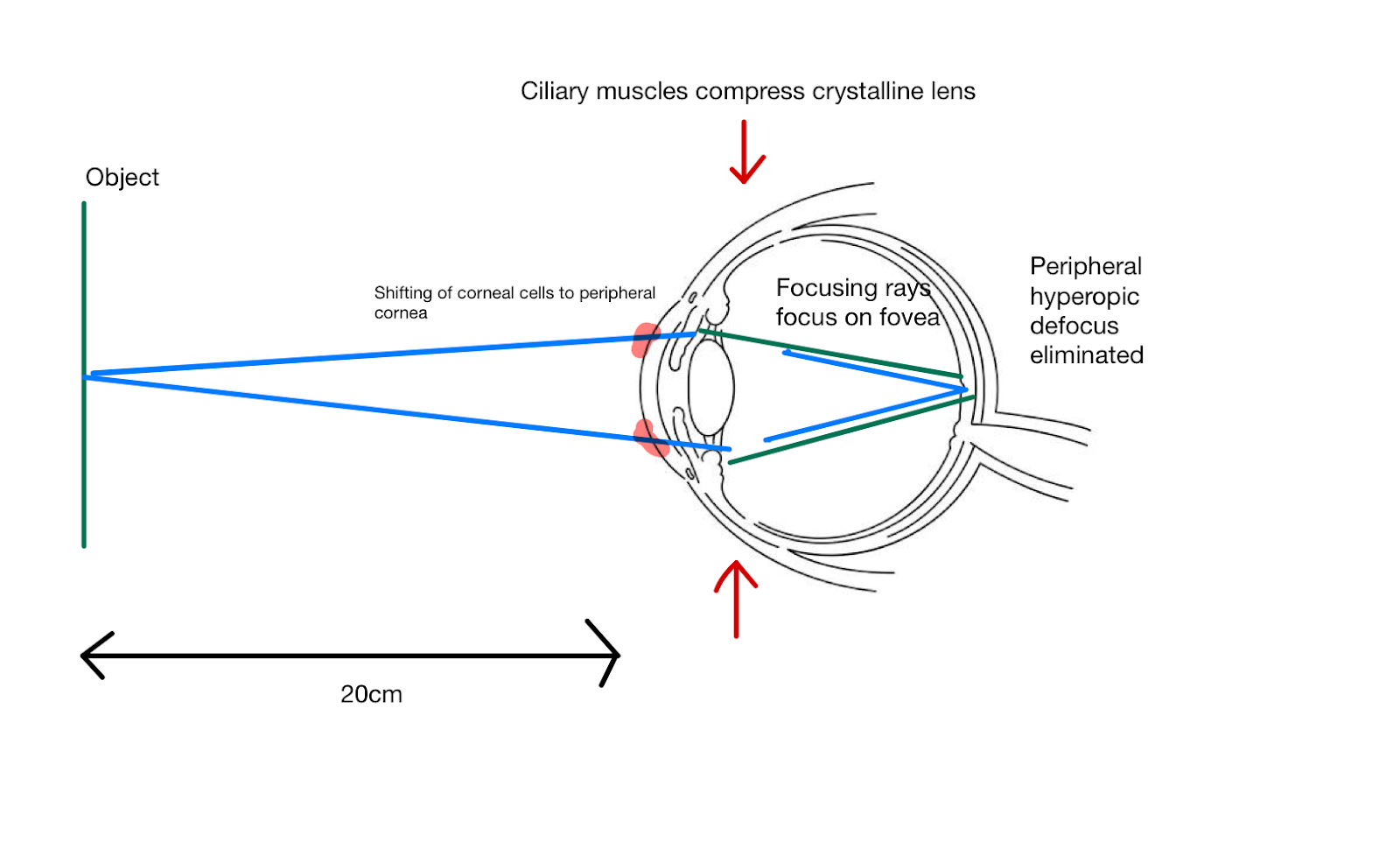
In this way, ortho-k lenses not only provides its user clear vision without the use of daytime spectacles or contact lenses, but also provides a two-pronged effect in slowing the progression of myopia.
Effectiveness in Myopia Control:
Now that we have established how ortho-k lenses could potentially reduce myopia progression based on its mechanism of creating a peripheral defocus zone, let's look at the evidence and its effectiveness of myopia control.
A randomized study conducted in 2012 showed that ortho-k lenses reduced axial elongation by 43% as compared to Single Vision Distance spectacles [3].
A separate study, published in 2024, showed a 39% decrease in axial elongation over a period of 2 years between children who used ortho-k and children who used Single Vision Distance spectacles [4]. In fact, 7.9% of children in the ortho-k group showed no axial elongation at all. This indicates a very high efficacy of myopia control in these groups.
While these studies show promising results of ortho-k and its effectiveness against the progression of axial myopia, it is important to note that efficacy levels vary between individuals; due to other factors such as age, handling of lenses, and lifestyle habits.
Handling:
Although an ortho-k program costs around S$2400 to S$2600 for a pair of lenses, ortho-k’s benefits of clear vision and myopia control may be enough to convince the discerning parent to enroll their child into an ortho-k program at their local Optometrist. However, when it comes to practicality, not everything about ortho-k is as smooth sailing as it seems.
Having a pair of hard lenses in your eyes while you sleep may not be the most comfortable experience. A child may quickly be discouraged to use ortho-k lenses if they are unable to bear the initial discomfort. Hence, a child has to be old enough to be suitable for ortho-k wear. They have to understand not only the importance of myopia control, but also that there will be an initial adaptation period to the discomfort of ortho-k lenses.
Moreover, a certain level of fine motor skill and hygiene level is needed to handle the contact lenses. Our recommended age for ortho-k is from 11 years old onwards.
One may consider other myopia control products in the industry, such as peripheral defocus spectacles in Hoya’s Miyosmart Lenses or Zeiss Myocare Lenses. Myopia control soft contact lenses in Coopervision’s MiSight Lenses may also be a good alternative to ortho-k lenses for daytime wear, especially for younger children.
Verdict:
Ortho-k lenses are indeed a unique piece of technology. There is no other type of technology that alters your vision during the night while you are sleeping, and ensures clear vision during the day. Although there are drawbacks such as initial discomfort and cost, nothing beats not having to wear spectacles or soft contact lenses during the day- especially for a child with an active lifestyle. On top of that, myopia is an irreversible condition, and controlling it is crucial in minimizing the risk of myopia-related eye diseases in the future. In my opinion, all these make the cost of ortho-k worth it. Nothing beats its benefits of effective myopia control and provision of spectacle-free clear vision.
References:
-
Biswas, S. et al. (2024) ‘The influence of the environment and lifestyle on myopia’, Journal of Physiological Anthropology, 43(1). doi:10.1186/s40101-024-00354-7.
-
Matsumura, S., Kuo, A.N. and Saw, S.-M. (2019) ‘An update of eye shape and myopia’, Eye & Contact Lens: Science & Clinical Practice, 45(5), pp. 279–285. doi:10.1097/icl.0000000000000571.
-
Cho, P. and Cheung, S.-W. (2012) ‘Retardation of myopia in Orthokeratology (romio) study: A 2-year randomized clinical trial’, Investigative Opthalmology & Visual Science, 53(11), p. 7077. doi:10.1167/iovs.12-10565.
-
Santodomingo-Rubido, J., Cheung, S.-W. and Villa-Collar, C. (2024) ‘A new look at the myopia control efficacy of Orthokeratology’, Contact Lens and Anterior Eye, p. 102251. doi:10.1016/j.clae.2024.102251.